Wound Bed Preparation- Debridement
The specific type of tissue present in the wound bed has a definite impact on healing. Tissue that is nonviable can delay healing and must be removed in order to allow healing to resume. It is important to make note of and document the type of tissue present in the wound when examining the wound in order to be able to determine whether the wound is healing over time. Nonviable tissue not only delays wound healing, but can also provide a locus of infection, in addition to prolonging the inflammatory phase and impeding epithelialization.
Necrotic Tissue Described
Necrotic tissue is simply dead tissue that is no longer viable. It is comprised of dead cells and debris. It changes color, becoming darker as the tissue becomes more dehydrated. Necrotic tissue may be subdivided into two types:
- Slough– slough is tan or yellowish in color. It has a mucous-like consistency and is often ‘stringy’ in appearance. It is composed of bacteria, extracellular matrix that has become degraded and white blood cells. It is often loosely adherent to the wound bed in comparison to eschar. It is thought to be associated with the presence of bacteria in the wound.
- Eschar– eschar is black and may be soft or hard. It is often firmly adhered to the wound bed and can be difficult to remove. As a general rule, the greater the depth of tissue destruction, the more adherent the necrotic tissue. Slough often lies on the surface, while eschar may form a thick, tenacious layer.
The characteristics of the tissue found in the patient’s wound bed should be described, and the percentage of the wound bed occupied by each tissue type should be measured and recorded at each patient visit.
The presence of necrotic tissue in the wound bed means that you cannot accurately assess the size and depth of the wound. Once necrotic tissue is removed, the wound may actually be much larger than initially suspected. The process of removing dead tissue is known as debridement. Before debriding a wound it is important to ensure that there is adequate blood flow to the area.
Types of Debridement
There are many ways to remove dead or devitalized tissue that is standing in the way of wound healing. The following are some of the most common ways:
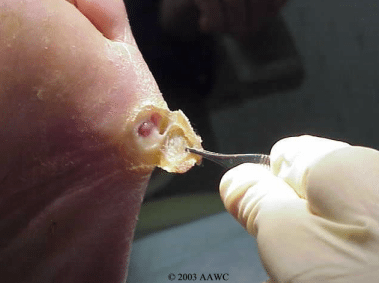
- Surgical debridement– this is one of the fastest ways of debriding a wound and is performed under sterile conditions, often in the OR under local or general anesthetic. Surgical debridement is usually reserved for large wounds when infection is a concern. Surgical debridement automatically converts a chronic wound into an acute wound.
- Sharp debridement– although usually more conservative than surgical debridement, large amounts of tissue may be removed. Sharp debridement, similar to surgical debridement, requires that the practitioner have expert knowledge of anatomy and the ability to manage any complications such as bleeding. Practitioners should not perform sharp debridement without the necessary skills and knowledge. Patient consent should be obtained, just as with surgical debridement.
- Autolytic debridement– this type of debridement uses the wound exudate advantageously to separate the necrotic tissue from viable tissue. The process can be helped along using occlusive and semi-occlusive dressings which interact with the wound bed to create a moist wound environment.
- Enzymatic debridement– this type of debridement can be used to assist in removal of hard necrotic tissue when the patient is not a candidate for surgical debridement. This method utilizes exogenous enzymes which react with wound bed enzymes to break down the necrotic tissue present. This method takes time.
- Biologic debridement (larval therapy) – maggots grown in a sterile environment are introduced into the wound, where they secrete enzymes that break down necrotic tissue, leaving the healthy tissue untouched. Although this method can be very effective, many people are squeamish about this method.
- Mechanical debridement– this method is rarely used nowadays, although it was popular in years past. This method involves the use of irrigation or wet-to-dry dressings to remove dead tissue. This method is not only painful, but can also remove newly granulated tissue along with the dead or devitalized tissue.
Along with management of infection and moisture in the wound bed, debridement is an important part of wound bed preparation and management. If you enjoyed this article and want to learn more about wound care, visit Wound Educators, the site dedicated to preparing professionals to become certified wound care consultants.
Sources:
Dowsett, C. & Newton, H. (n.d.). Wound Bed Preparation: TIME in Practice. Wounds International. http://woundsinternational.com/pdf/content_86.pdf
Dowsett, C & Schultz, G. (2012). Wound bed preparation revisited. Wounds International, February 3(1).
My sister has wounds in her legs severely like that. But she also has bursitis of the hip and neuropathy. She cannot elevate her legs due to pain in her hip. She needs a hip replacement but the infection in her legs have to be dealt with first. Is there something that could be done with the hip to relieve the pain so she could Elevate her legs which will help the wounds in her legs go away?